DOI: 10.26717/BJSTR.2023.53.008337
National University of Physical Education and Sports, Faculty of Physical Education and Sport, Romania.
*Corresponding author: Alexandra Tufa, National University of Physical Education and Sports, Faculty of Physical Education
and Sport, Bucharest, Romania
Received: August 28, 2023
Published: September 26, 2023
Citation: Alexandra Tufa and Silvia Te- odorescu. The Importance of Physical Therapy in Increasing the Quality of Life of Women with Urinary Incontinence Through Static and Dynamic Reeduca- tion Methods. Biomed J Sci & Tech Res 53(1)-2023. BJSTR. MS.ID.008337.
Urinary incontinence has a major impact in terms of quality of life, environmental, economic and health. This work aims to highlight the importance of physical therapy in increasing the quality of life, improving or treating the symptoms of women with urinary incontinence through static and dynamic reeducation methods. 64 women with stress urinary incontinence, in some cases associated with urination emergencies, prolapse or incontinence, were studied. They were divided into two groups, 32 patients in the “static” group and 32 patients in the “dynamic” group. In the dynamic group, reeducation was achieved by associating electrostimulation and biofeedback with dynamic exercises. In our article, we develop a factor analysis based on structural equation model utilizing Smart PLS software. The results showed that physiotherapeutic methods help increase the quality of life and improve or treat urinary incontinence through both static and dynamic reeducation methods. Both groups performed satisfactorily, but the static group performed slightly better than the dynamic group. In conclusion, dynamic reeducation is recommended to be introduced progressively in the second part of kinetic treatment.
Keywords: Urinary and Fecal Incontinence; Physiotherapy; Biofeedback Dynamic
Abbreviations: UI: Urinary Incontinence; ICS: International Continence Society; IUM: Mixed Urinary Incontinence; IUU: Emergency Urinary Incontinence; PFD: Pelvic Floor Dysfunction; POPs: Pelvic Organ Prolapse; SEM: Structural Equation Modeling; PLS: Partial Least Squares; CFA: Confirmatory Factor Analysis; MPP: Perineo-Pelvic Musculature
Urinary incontinence (UI) has been defined by the International Continence Society (ICS) as «a condition in which urine loss is a social or hygiene problem and is objectively demonstrated» [1]. This definition was amended in 2002 by ICS, then adapted as «complaint of any involuntary leakage of urine» [2,3]. UI is an involuntary loss of urine that can occur at any age and has multiple causes. Sometimes urinary incontinence can be associated with incontinence, urgent urination needs, prolapse or sexual dysfunction. UI has a considerable impact on quality of life and, due to its high frequency in the general population, constitutes a major public health problem with a strong economic impact [4]. This work aims to highlight the importance of physical therapy in increasing the quality of life, improving or treating symptoms of women with urinary incontinence through static and dynamic reeducation methods. Biofeedback, electrostimulation and physical exercises are used to re-educate the pelvic floor muscles and help patients, by visualizing the perineal contraction on the screen, become aware of perineal muscle contraction and relaxation. They learn to control/train their corresponding muscle groups through increased awareness.
Urinary incontinence can be classified as SUI stress urinary incontinence, emergency urinary incontinence (IUU) or mixed urinary incontinence (IUM) [5]. SUI is defined as the involuntary leakage of urine during exertion, such as coughing, sneezing, laughing or physical activity. A sudden increase in abdominal pressure due to physical exertion puts pressure on the bladder, causing urine loss. The basic mechanisms responsible for this reaction are weak urethral support by the pelvic floor muscles and sphincter deficiency. IUU (commonly referred to as an «overactive bladder») is the involuntary leakage of urine associated with «urgency» [6] or a strong and sudden need to urinate. This incontinence is usually caused by involuntary contractions of the detrusor muscle of the bladder wall without the bladder necessarily being full. UUI can also be sensitive, i.e., it can be triggered by simple everyday events, such as the sound of running water, exposure to low temperatures or consumption of cold drinks [7]. The upper limit of urination during waking hours has been determined by the International Incontinence Society to be 7 urinations, although it may be higher in certain populations [8].
Urinary and faecal incontinence have a major impact ecologically, economically, health through urinary infections [9] and skin disorders [10] psychologically and socially through decreased quality of life. [11,12]. Most manufacturers of sorbents are looking for eco- responsible and effective solutions, but the large-scale use of sorbents has a significant negative impact on the planet.
The economic and social impact of incontinence is difficult to estimate, first of all, due to the lack of a real percentage of the incidence of this condition, of the direct costs (the cost of medical and therapeutic consultations, the costs of hospitalizations, absorbent protections…) and secondly , due to the indirect costs arising from incontinence: institutionalization of elderly people, absenteeism and performance at work, psychological disorders, depression [13]. Among athletes, it has been shown that there is an increased percentage of urinary incontinence, often poorly reported to the coach, parents or doctor. According to several studies, the percentage of exercise urinary incontinence among athletes or people who practice strenuous physical activities can reach a value between 28% and 80%. The sports with the highest risk are those that have repeated impacts with the ground: trampoline, gymnastics, hockey, ballet, jumping, etc. [14-18]. Pelvic floor dysfunction (PFD) is common after delivery, with approximately 30% of mothers experiencing urinary incontinence (IU) and 10% incontinence (AI) [19]. Urinary incontinence is sometimes associated with faucal incontinence, which is defined by the International Continence Society as the involuntary loss of faces or gas. Rectal contents (feces, gas) involuntarily pass through the anal canal and the patient is unable to postpone an evacuation until it is socially convenient. Attached to the definition, there is a time component of at least one month and an age of at least 4 years with previously achieved defecator control [20,21].
Depending on the circumstances fecal incontinence is classified as: passive incontinence (involuntary discharge without any awareness); incontinence by urgency (urgent needs and discharge despite active attempts to retain contents); faucal infiltration or «soiling» (leakage of faces often liquid, even after normal discharge) [22]. Urination emergencies, sexual dysfunction, pain, and pelvic organ prolapse (POPs) may also occurin association to the urinary or faecal incontinence. Between 40-91% of women in the first postpartum year may experience one or more of the perineal associated dysfunctions [23]. Prolapse symptoms (POPs) are a change from the normal sensation, structure, or function experienced by a woman relative to the position of her pelvic organs. Symptoms are generally worse at times whilst gravity could worsen prolapse (for example, after long periods of standing or exercising) and in certain cases more advanced even when gravity is not a factor, for example, in dorsal decubitus. Prolapse may be more prominent during periods of abdominal exertion, for example, during defecation [24].
The research addressed a number of 64 patients diagnosed with urinary incontinence (UI), respectively stress urinary incontinence (IUM), emergency urinary incontinence (IUU) or mixed urinary incontinence (IUM), sometimes associated with problems of pelvic statics (prolapsus), with faecal anal incontinence or gas. The patients presented this condition as a result of a vaginal birth, as a result of intense sports, due to hormonal deficiency during the peri-menopause period, multiple vaginal births, etc. The research participants were divided into 2 groups: 32 patients in the static group and 32 patients in the dynamic group. Patients come to the office under the guidance of family doctors or specialists in the region with a medical prescription for perineal re-education. This contains the patient›s diagnosis and in some cases the number of recommended sessions. However, most medical prescriptions leave the number of recommended sessions to the discretion of the physiotherapist depending on the evolution and particularities of the patient. In order to reach the aim of this study, the kinetotherapeutic means, the number and frequency of the sessions were selected in accordance with the medical antecedents, the motivation and the evolution of the patients.
Of the 312 patients who were presented to the clinic, 108 met criteria 1 and 2, whereas only 64 met all 5 criteria. The study was carried out between January 2022 and March 2023 in Minos, France, in the Kalta Physiotherapy Clinic using two electrostimulation and biofeedback devices Phenix Nano Physio, and the re-education materials necessary to perform the associated physical exercises. Intra-cavitation methods are performed using a Periform or Saint Cloud OVA vaginal probe, and the Anuform probe was used for anal re-education. To facilitate insertion of the probe and for electrical conductivity, a small amount of sterile water-based lubricating gel is applied to the electrodes of the probe before insertion. The physical therapy office is equipped with 5 individual rooms with a massage/ examination table and a gym. The materials used to perform physical exercises associated with intra-cavitation methods were mattress, gym-ball, bicycle, trampoline, treadmill, rope, stepper, half-sphere, proprioception balls.
The research contains:
with the intracavitary method were progressive and adapted to each patient, the goal of the dynamic group was to gradually train the pelvic floor in the position or situation as close as possible to the real situation/similar to the moments of urinary loss in daily life.
The fast fibers are in proportion of 30% of the perineum muscles and it will be trained through strong and short contractions with an intensity of 80%-100% for a duration of 2-5 seconds. Slow fibers predominate in proportion to 70% because they ensure urinary and fecal continence through prolonged contraction of the urinary and anal sphincter. They will train with an intensity between 50%-70% for a duration of 5-15 seconds. Abdominal-perineal contractions are recommended to be performed on exhalation or in the case of prolonged contractions, if the patient feels the need, a nasal inhalation can be performed and emphasis will be placed on a prolonged oral exhalation as slowly as possible, resuming normal breathing during breaks. Each session lasts approximately 30 minutes.
and 33 Hz with a wavelength between 320 and 740 μs.
and 80 Hz with a wavelength between 20 and 160 μs.
Smart PLS is a software tool that provides a straightforward user interface for doing SEM analysis. It is designed primarily for Partial Least Squares (PLS) route modeling, which is a variance- based SEM approach. Researchers can use PLS-SEM to analyze the structural model (relationships between latent variables) and Smart PLS to evaluate the measurement model (reflective and formative indicators). Confirmatory Factor Analysis (CFA) is a statistical approach that assesses the measurement properties of a set of observable variables (indicators) and their relationships to latent variables (constructs). It is a confirmatory factor analysis approach in which researchers construct a hypothesized component organization based on theory or previous studies and then contrast it to the data that was observed. CFA is used to determine how well the proposed measurement model fits by examining the factor loadings, errors in measurement, and general model fit indices. Path analysis serves as a method for determining whether variables in a theoretical framework are causally connected. It allows researchers to assess both short- and long-term interactions among factors. Path analysis computes a number of equations for regression at the same time to examine the relationships between variables. Researchers may analyze the coefficients of the variables to determine the degree and significance of the directional relationships (paths) between them.
The present research is structured on several levels, materialized by using research tools meant to provide a comprehensive perspective on urinary incontinence, focusing on the analysis of the impact of this phenomenon on the symptomatology and quality of life before and after physiotherapy treatment. The study uses the longitudinal method, providing a temporal image of this pathology, being applied research tools that allow the comparison of data, before and after performing kinesitherapy procedures. The analysis of the data shows some characteristics of patients (Table 1) thus, the average age of patients is 46.5 years, the youngest being 18 years and the oldest 78 years. The most common age throughout the sample is 57 years, in the dynamic group 54 years, and in the static group 57 years. The average BMI of patients is 25.9, the lowest BMI is 18 and the highest is 42.6. Next, we analyzed the relationship between BMI and symptomatology. It highlights the fact that the highest BMI values, above 30, often cause urinary incontinence associated with prolapse. The duration average of this pathology in the analyzed sample is 4 and a half years, most commonly women have this condition of 1 year, and the longest time for experiencing urinary incontinence is 42 years. The average of births per patient is 2, the number of births most commonly found in the static group is 2, and in the dynamic group is one. We notice that the number of births also influences the symptomatology, the highest values in terms of symptoms, presenting patients who gave birth to 3 children.
The present research is structured on several levels, materialized by using research tools meant to provide a comprehensive perspective on urinary incontinence, focusing on the analysis of the impact of this phenomenon on the symptomatology and quality of life before and after physiotherapy treatment. The study uses the longitudinal method, providing a temporal image of this pathology, being applied research tools that allow the comparison of data, before and after performing kinesitherapy procedures. The analysis of the data shows some characteristics of patients (Table 1) thus, the average age of patients is 46.5 years, the youngest being 18 years and the oldest 78 years. The most common age throughout the sample is 57 years, in the dynamic group 54 years, and in the static group 57 years. The average BMI of patients is 25.9, the lowest BMI is 18 and the highest is 42.6. Next, we analyzed the relationship between BMI and symptomatology. It highlights the fact that the highest BMI values, above 30, often cause urinary incontinence associated with prolapse. The duration average of this pathology in the analyzed sample is 4 and a half years, most commonly women have this condition of 1 year, and the longest time for experiencing urinary incontinence is 42 years. The average of births per patient is 2, the number of births most commonly found in the static group is 2, and in the dynamic group is one. We notice that the number of births also influences the symptomatology, the highest values in terms of symptoms, presenting patients who gave birth to 3 children.
Table 1: Data on research participants.
The current patient’s age | Patient’s age the at the UI occurrence | UI duration (year) | UI Stadium | BMI | No of births | No of hours/ week sports | |
Total Avg | 46.5 | 41 | 4.5 | 1.8 | 25.9 | 2 | 2.7 |
Dinamic Avg | 49.4 | 42.8 | 5.6 | 1.9 | 26.4 | 2 | 2.5 |
Satic Avg | 43.6 | 39.1 | 3.5 | 1.7 | 25.3 | 2 | 2.9 |
Minim total | 18 | 10 | 0 | 1 | 18 | 0 | 0 |
Minim Dynamic | 26 | 15 | 0 | 1 | 18.8 | 0 | 0 |
Minim static | 18 | 10 | 1 | 1 | 18 | 0 | 0 |
Maxim total | 78 | 77 | 42 | 3 | 42.6 | 4 | 12 |
Maxim Dynamic | 78 | 77 | 42 | 3 | 38.1 | 4 | 12 |
Maxim statice | 72 | 64 | 12 | 3 | 42.6 | 4 | 10 |
Mode total | 57 | 49 | 1 | 2 | 27.3 | 2 | 0 |
Mode Dynamic | 54 | 35 | 1 | 2 | 30.4 | 1 | 0 |
Mode static | 57 | 46 | 3 | 2 | 24.2 | 2 | 0 |
Below are presented the number of hours per week of sports activities practiced by the research participants, the average being
2.7 hours per week, 2.5 hours per week for the dynamic group and
2.9 hours per week for the static group. The type of physical activity was analyzed according to the symptoms, so the respondents have a series of varied activities, most of them being oriented towards walking, biking, fitness, running and tennis. However, we notice that 33% of patients do not practice any physical activity and represent the highest share in terms of symptoms. It appears, however, that cycling has a major impact on urinary incontinence associated with gas incontinence. We also analyzed kinetic treatment (Table 2) according to the number of sessions performed, duration and frequency, whether exercises were performed at home and with what frequency. Frequency was measured from a scale of 1 to 5 (1=less than once a week, 2= once a week, 3= twice a week, 4= three times a week, 5= more than 3 times a week). The duration of a home reeducation session was measured on a scale of 1 to 4 (1 = less than 5 minutes, 2 = 5-10 minutes, 3 = 10-15 minutes, 4 = more than 15 minutes). Next, we analyzed the impact of urinary incontinence on the quality of life perceived by the respondents by applying a research tool to measure how the therapy positively impacted the daily life of the patients. Thus, a pre-test and post-test questionnaire was used to be able to observe how there were changes in the quality of life throughout the therapy.
Table 2: Information on kinetic treatment.
Intervention Program | Number of sessions | Duration (months) | Frequency of sessions | Frequency of self- exercises | Duration of self- exercises |
Avg total | 16.2 | 4.5 | 2.2 | 1.8 | 1.8 |
Avg dynamic | 16.8 | 4.7 | 2.2 | 1.6 | 1.8 |
Avg static | 15.5 | 4.4 | 2.3 | 1.9 | 1.8 |
Minim total | 8 | 2 | 1 | 0 | 0 |
Minim dinamic | 8 | 2 | 1 | 0 | 0 |
Minim static | 8 | 2 | 1 | 1 | 1 |
Maxim total | 45 | 12 | 4 | 6 | 4 |
Maxim dynamic | 45 | 12 | 3 | 4 | 4 |
Maxim static | 25 | 12 | 4 | 6 | 4 |
Mode total | 15 | 2 | 2 | 1 | 1 |
Mode dynamic | 15 | 2 | 3 | 1 | 1 |
mode static | 15 | 3 | 2 | 2 | 1 |
The analyzed data presents a general picture related to aspects of the personal life of the respondents such as the impact of IU on social, intimate, psychological and the quality of life (Contilife questionnaire). The calculation of the means at the initial and final testing was done on a scale from 0 (not at all) to 3 (strong impact) and on a scale from 0 (not at all) to 5 (strong impact) for the Contilife questionnaire. Contilife questionary describes daily activities, effort situations, self-image, emotional outing, sexuality and wellbeing. An increased difference in the scores obtained for all dimensions of life analyzed is observed. The symptoms that appear during various activities, such as playing sports, laughing, shopping, climbing stairs, etc., have a great impact at a social, intimate and psychological level, the patient developing different fears such as that of not being seductive anymore, of smells, of incontinence during sexual activity, soiling clothes, etc.
Analyzing the very strong positive correlation between activities and fears (0.937), activities and impact (0.868), fears and impact (0.873), according to the data in (Table 3), results in the model in (Figure 1), which represents the graphic expression that confirms that urinary incontinence decreases patients› quality of life. In this model the correlation coefficients are equal to the path coefficients (Table 3). Our model contains 3 variables: Activities, Impact and
Fears, each characterized by several items shown in (Figure 1). The Activities variable consists of 9 items (Figure 1), among which those with the highest weight are IU outside (LF=0.850), Shopping (LF=0.786), Sneezing and Laughing (LF=0.753), Extended Wait (LF= 0.625), Sports practicing (LF=0.622), Stairs climbing (LF=0.592), Lifting objects (LF=0.592) and UI in means of transport (LF=0.519). These represent the activities carried out by the patients in which the symptom of urinary incontinence occurs with a greater frequency. The Impact variable consists of 9 items (Figure 1), among which those with the highest weight are Straining (LF=0.844), Psychological Impact (LF=0.808), Social Impact (LF=0.799), Intimate Impact (LF= 0.782), Urinary control (LF=0.729), loss of patience (LF=0.622), Discouragement (LF=0.597), Obsession (LF=0.495), Use of absorbent pads (LF=0.490). Thus, we can analyze/observe to what extent the patients are affected by urinary incontinence. We notice that subtle or invisible factors such as Discouragement, Obsession, wearing absorbent pads are ranked last.
Table 3: Latent Variable Correlation.
Activities | Fears | Impact | |
Activities | 1 | 0.937 | 0.868 |
Fears | 0.937 | 1 | 0.873 |
Impact | 0.868 | 0.873 | 1 |
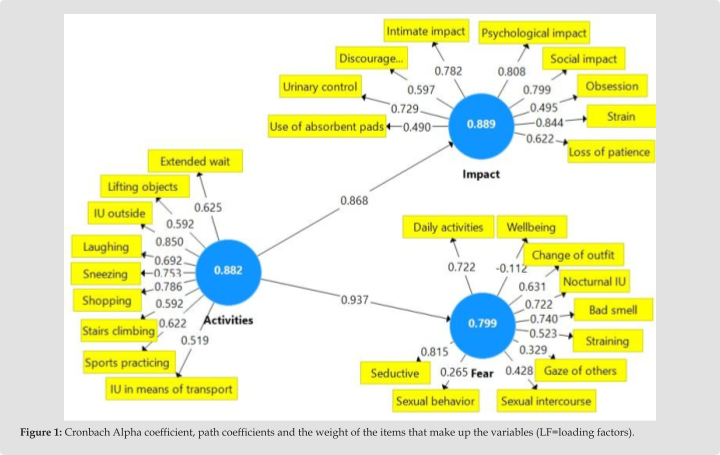
The Fears variable consists of 10 items referring to different fears of the patients (Figure 1), of which the ones with the highest weight are the fear of not being seductive anymore (LF=0.815), Bad smell (LF=0.740) – the fear of smelling, nocturnal UI (LF=0.722) – Incontinence or fear of Waking up wet at night, Daily activities (LF=0.722) – having to interrupt certain activities either at work or in free time, Change of outfit (LF=0.631) – the patient had to change her outfit, Staining (LF=0.528) – fear of staining herself, Sexual Intercourse (LF=0.428) – damage to intimate relationships. The only negative Item is Wellbeing (LF=-0.112) nevertheless the Conti life questionnaire offers a distorted value which suggests a negative evolution whereas it actually suggest an improvement of it. There are authors who state that variables with negative values must be excluded from the model. Other authors state that they can decisively influence the model. We decided to keep the variable because it confirms the real situation of the patients. The load factors (LF) presented above and the high value of the R Square coefficient for Fears (0.879) and Impact (0.753) demonstrate that the factors/items that form each variable are representative of the model and that they should be included in the history of patients with UI. The Adjusted R Square value (Table 4) reveals that only 87.7% of the variance of the dependent variable (Fears) is explained by the variance of the independent variable (Activities) and that only 74.9% of the variance of the dependent variable (Impact) is explained by the variance of the independent variable (Activities). The Chi-Square value of the estimated model (872,821) is higher than the minimum threshold of the saturated model (870,958), as a result, our model is validated (Table 5).
Table 4: Square R metrics.
R Square | R Square Adjusted | |
Impact | 0.879 | 0.877 |
Fears | 0.753 | 0.749 |
Table 5: Chi-Square Values.
Saturated | Estimate | |
Chi-Square | 870.958 | 872.821 |
Smart Pls software offers many tests that can be used to ensure a consistent factorial analysis and interpretation of data and to take ownership of research results. For example, the consistency of our model was based on the validation steps set out in (Table 6). All variables show a high value for the reliability of the model Composite
Reliability (>0.6), Cronbach Alpha and rho_A (> 0.7 – the minimum accepted value). We note that for our model these indicators have very high values, which validates the relationship between variables and the weight of influence of each variable. The subitems that form the variables are defining and relevant, as can be seen from the large weights (LF) in (Figure 1) and the large value of Cronbach›s Alpha Coefficient. In our case, the model is correctly designed because all indicators validate CA, rho_A and CR are higher than even 0.8, for all 3 variables (Table 7).
Table 6: Indicators validating the model.
Cronbach’s Alpha | Rho_A | Composite Reliability | |
Activities | 0.882 | 0.892 | 0.882 |
Fears | 0.799 | 0.863 | 0.793 |
Impact | 0.889 | 0.906 | 0.892 |
Table 7: Multicollinearity analysis.
Variables | VIF | Variables | VIF | Variables | VIF | Variables | VIF |
Use of absorbents pads | 1.644 | UI outside | 2.962 | Obsession | 1.284 | Loss of patience | 2.553 |
Daily activities | 2.056 | Change of outfit | 1.95 | Strain | 2.16 | Climb stairs | 2.411 |
Wellbeing | 1.194 | UI Nocturnal | 1.346 | Concern | 3.921 | Seductive | 2.358 |
Extended wait | 3.44 | Intimate impact | 1.928 | The gaze of others | 1.536 | Sexual behavior | 2.473 |
Urinary control | 4.631 | Psycho impact | 2.957 | Intimate relationships | 3.316 | Sports | 1.861 |
Shopping | 4.597 | Social impact | 1.938 | Lifting objects | 1.574 | Sneeze | 2.372 |
Discouragement | 3.495 | Bad smell | 2.755 | Laughing | 2.856 | Transport | 1.575 |
The inflation change factor (VIF) of each variable was calculated to check the significance of the variables. (Table 8) shows the VIF values associated with each variable. All values are less than 5, which denotes almost no collinearity. Relating initial perceptions of UI timing to opinions expressed in final testing, on a scale of 1 (never) to 5 (every day) it follows that individuals who gave high values of UI intensity at initial testing consider that UIs are less common today (Table 8). To find out if there is a statistically significant difference between the mean of the frequency of urinary incontinence at the initial and final testing we apply the T-test. Significant differences are observed for the initial and final values for the Dynamic Group and the Static Group, the Tstat value of the test is 6.93 for the group dynamic and 31 for the static group is greater than the minimum accepted Critical two-tail t value (2.04), with a very high level of significance (p=0.00<0.05) and a confidence level of 95%. We conclude that the difference between the test means is statistically significant. The statistical inference test allows us to extrapolate our conclusion to the entire statistical population, because t Stat > t Critical and p<0.05. The mean frequency of urination in the dynamic group decreased from 4.28 to 2.59, and in the static group from 4.56 to 1.90. Next, the initial and final contraction force was analyzed using the intravaginal probe and the biofeedback device. A significant increase in contraction force was observed for the entire population with an average of 54%, an average evolution of 60% in the static group and 48% in the dynamic group (Table 9).
Table 8: Initial/final UI frequency across sample and two groups.
UI Frequency | Total echelon | Static Group | Dinamic Group | ||||||
Initial | Evolution | Final | Initial | Evolution | Final | Initial | Evolution | Final | |
Average | 4.42 | -49% | 2.27 | 4.56 | -58% | 1.91 | 4.28 | -40% | 2.59 |
Minim | 2 | -50% | 1 | 1 | 0% | 1 | 2 | -50% | 1 |
Maxim | 5 | 0% | 5 | 5 | -100% | 5 | 0% | 5 | |
Mode | 5 | -60% | 2 | 5 | -60% | 2 | 5 | -60% | 2 |
Table 9: Initial and final biofeedback contraction force on the whole sample and the two groups.
Contraction force BFB | Total echelon | Static Group | Dinamic Group | ||||||
Initial | Evolution | Final | Initial | Evolution | Final | Initial | Evolution | Final | |
Average | 23.39 | 54% | 36.03 | 24.45 | 60% | 39.17 | 22.44 | 48% | 33.19 |
Minim | 2 | 250% | 7 | 3 | 333% | 13 | 2 | 250% | 7 |
Maxim | 53 | 23% | 65 | 53 | 23% | 65 | 48 | 35% | 65 |
Mode | 23.39 | 62% | 38 | 24.45 | 104% | 50 | 22.44 | 7% | 24 |
To find out if there is a statistically significant difference between the mean biofeedback contraction force at the initial and final testing we apply the T-test. Significant differences are observed for the initial and final values for the Dynamic Group and the Static Group, The Tstat value of the mode test is 6.30 for the dynamic group and 9.46 for the static group is greater than the minimum accepted Critical two-tail t value (2.04), with a very high level of significance (p=0.00<0.05) and a confidence level of 95%. We conclude that the difference between the test means is statistically significant. The statistical inference test allows us to extrapolate our conclusion to the entire statistical population because t Stat > t Critical and p<0.05. The average biofeedback in the Dynamic Group increased from 22.44 to 33.19, and in the Static Group from 22.26 to 35.50. To find out if there is a statistically significant difference between the mean on the impact of urinary incontinence on quality of life at the initial and final testing, we applied the T-test. Significant differences are observed for the initial and final values for the Dynamic Group and the Static Group, The Tstat value of the test in module is 7.57 for group 1 and 9.18 for group 2, is greater than the minimum accepted value t Critical two- tail (2.04), with a very high significance level (p=0.00<0.05) and 95% confidence. We conclude that the difference in test environments is statistically significant. The statistical inference test allows us to extrapolate our conclusion to the entire statistical population, since t Stat > t Critical and p<0.05.
The average negative impact in the Dynamic Group decreased from 2.11 to 0.95 and in the Static Group from 1.84 to 0.63. The kinetic program through reeducation methods (Reeducation methods) and sessions already performed previously by patients through sessions prior to current treatment (Prior reeducation) helps to increase perineal muscle strength (Final BFB contraction force), improve or disappear urinary leakage symptoms (Final IU frequency) and increase quality of life. Among the quality-of-life items, those who had the greatest improvement were: Activity interruptions, Activities Impairment, fears, urinary problems, sexual behavior and use of absorbent pads (Figure 2). Path analysis coefficients demonstrate that the reeducation methods used and prior reeducation increased perineal muscle (performance lf = 0.206) and quality of life (quality of life 0.380) (Figure 2). The Cronbach Alpha coefficient 0.755 (Figure 2) shows that variables in the analysis were suitable for designing the model. In the analysis were introduced 2 formative variables (reeducation and performance) and one reflective (quality of life). The weight of the reeducation variable denotes that the highest impact was obtained by the reeducation methods with a high charging factor (lf = 0.720). And the reeducation previously played a role in increasing the strength and quality of life, but to a small extent (lf = 0.570). The formative variable performance consists of 2 subitems final contraction force BFB with a very high charging factor Lf = 0.953 and final IU frequency (lf = 0.478). This fact denotes that the final biofeedback force has had the highest share in the evaluation. However, the frequency of IU/urinary losses has improved (decreased).
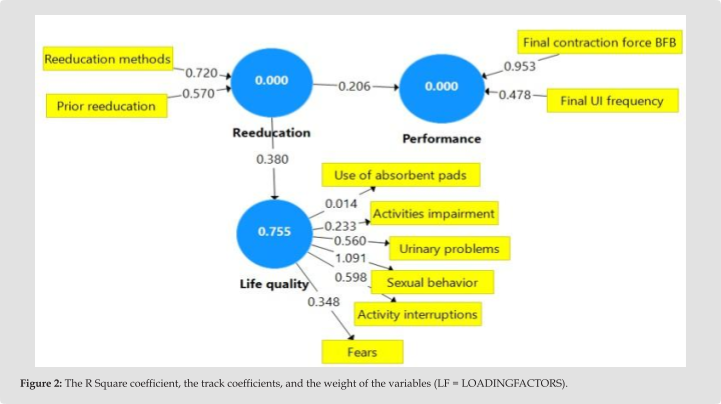
Sexual behavior with a very high load factor LF=1.091 has been cured to a very large extent and refers to 3 elements: Does the thought of having sexual intercourse concern you? Have you changed your sexual behavior? Are you afraid that you will leak urine during sexual intercourse? Urinary problems (LF=0.560) have been largely cured and refer to moments of discouragement, loss of patience, fear of urinary problems and lack of control in this regard, urinary problems becoming an obsession or anxiety, as well as wearing pads. Activity Interruptions (LF=0.598) – patients no longer have to interrupt certain activities or at work or during their free time. Activities Impairment (LF=0.233) – the sensation of micturition diminished when patients perform certain outdoor activities, in means of transport, on stairs, shopping or when waiting in line / shopping. Fears (LF=0.348) of being a little seductive, of smelling, of looking at others, of staining oneself, of having to change clothes have decreased, and general well- being has increased. Use of pads (LF=0.014) patients are forced to wear pads less and less.
The SmartPls software offers many tests that can be used to ensure a coherent factor and interpretation of data and to assume the results of the research. For example, the coherence of our model was based on validation steps provided in (Table 10). Life quality has a high value for the reliability of the composite= 0.626 (> 0.6), Cronbach Alpha (0.755) and Rho_a (0.829) greater than 0,07 the minimum authorized threshold. We notice that for the variables of contraction and reeducation, the model only calculates the rho_a values, because they are formative variables. In our case, the model is correctly designed because all indicators validate it (Table 11).
Table 10: Chi Square coefficient.
Saturated Model | Estimated Model | |
Chi-Square | 195.893 | 197.239 |
Table 11: Model validation steps.
Cronbach’s Alpha | Rho_A | Composite Reliability | |
Life quality | 0.755 | 0.917 | 0.671 |
Performance | 1 | ||
Rehabilitation | 1 |
Our model is statistically powerful, because the Fornell-Larcker criterion is met. The 3 variables represent different concepts that do not overlap with any sudden (Table 12). The Chi Square coefficient of the estimated model (197.239) is higher than the Square›s coefficient of saturated model (195,893), so our model has a very high prediction power (Table 10).
Table 12: The Fornell-Larcker criterion.
Life quality | Performance | Rehabilitation | |
Life quality | 0.583 | ||
Performance | 0.139 | ||
Rehabilitation | 0.38 | 0.206 |
The factor of variation of inflation (VIF) of each variable has been calculated using 5000 samples and a 95% bootstrapping procedure to verify the significance of variables. All values less than 5 express an extremely low collinearity. Values lower than 3 non -existent collinearity. (Table 13) presents an overview of the findings. Thus, we can declare that the Global VIF does not have multicollinearity between variables. Following the kinetic treatment, we observe an increased satisfaction of patients. On a scale from 1 (not at all) to 5 (huge), 48% are satisfied, 21% are very satisfied, 15% are quite satisfied, 9% are a little satisfied and only 0.01% are not satisfied. The most increased satisfaction being in the age categories under 20 years with a value of 5, as well as in persons over 70 years, with an average value of 4.3.
Table 13: Analysis of multicollinearity.
VIF | VIF | ||
Use of absorbent pads | 1.047 | Activity Interruptions | 2.114 |
Activities Impairment | 2.833 | Rehabilitation methods | 1.038 |
Final BFB contraction force | 1.023 | Urinary problems | 2.127 |
Sexual behavior | 1.369 | Prior reeducation | 1.038 |
Final frequency | 1.023 | Fears | 1.457 |
Dysfunction of the pelvic floor muscles and the sequelae of birth trauma on it cause distress and reduce quality of life, including reduced participation in physical activity and exercise [25-26]. Pelvic floor muscle training (PFMT) in the female population has a level of proof of 1A for success in treating UI and is recommended as a first-line treatment [27,28]. In treatment management, as a rule, the first choice should be the least invasive method with the least adverse effects and complications for the patient. In this context, behavioral techniques and pelvic floor muscle training techniques meet these criteria for most forms of urinary incontinence. The pelvic floor is an organ with permanent reactivity [29]. It must be viewed in its anatomical and physiological globality, being a permanent adaptation structure, depending on the abdominal pressures and the physiological function (respiratory movements, physical efforts, etc.). It can be a primary cause in the imbalances of pelvic static and prolapse. In order to ensure an appropriate contractile response to any potential disturbing factor, a muscle must be permanently ready to react. Thus, a functional pelvic floor at rest is positioned, somewhere in the middle of the amplitude of its movement race, so in the average area. He returns to this average rest position when he relaxes, following a voluntary contraction. In order to maintain this average position against gravitational and abdominal strength, the pelvic floor muscles must have a permanent tonic activity. Therefore, from a histological point of view, these muscles are made up mainly of type I fibers, that is, slow and long contractions, which are hard to tire, and resist effort [30].
This is important in choosing electrostimulation currents and physical exercises within the reeducation of focus on stimulating slow fibers. The proposed physical exercises will be performed by the patients at home/ gym and after the end of the reeducation treatment both to maintain the result obtained and to prevent the occurrence of possible relapses. The perineum is a muscle like any other and its muscle tonicity is maintained by regular workouts. Within the dynamic reeducation, there are numerous combinations of physical exercises associated with electrostimulation and biofeedback, but they must be adapted to each patient, so that its level of physical training is respected and in no case should there be urinary incontinence during exercises. If one of the exercises causes urine leakage, it means that the perineo-pelvic musculature (MPP) is not yet tonic for that stage, we return to the previous stage. Also, in the early dynamic reeducation I have noticed that patients are much harder to raise awareness of the perineal contraction, their attention being more focused on physical exercise than on the abdominal-perineal contraction. Therefore, an
«automation» of the abdomio-perineal contraction is recommended before its association with dynamic physical exercises. In the case of athletes or women with intense physical activity who have urinary incontinence associated with prolapse, it may be recommended to wear a cube-shaped pessary to provide mechanical support during efforts [31].
It will act as a «splint» that will support the walls of the vagina, with the purpose of relieving prolapse [32] and urinary incontinence symptoms by avoiding urethral hypermobility or lowering the bladder, thus putting pressure on the sphincter or even causing bladder hyperactivity. Following the documentary research in the national and international literature, we noticed that the «fixed» variable was the number of physiotherapy sessions or certain reeducation techniques. In this research, we prioritized the patient and the improvement or treatment of symptoms. The number of sessions and the reeducation technique were chosen according to this, the priority being to adapt the physiotherapeutic means according to the particularities of the disease and evolution and not just to impose a standardized protocol established in advance. Therefore, the research is retrospective, the variable number of sessions and the physiotherapeutic means have been adapted according to the evolution of the patient, the improvement of symptoms and the regaining her quality of life. In the branch of perineal reeducation, therapists often choose a single method of re -education: only manual reeducation, only electrostimulation or biofeedback or just the physical exercise method. Often a single method can have satisfactory
results, but it presents certain limits. Therefore, it is important to combine these techniques to provide patients with a complete, long -term re -education with the recommendation to continue the
«for home» protocol or in the case of athletes to integrate physical exercises in sports training for maintaining muscle tonicity and lowering risk of relapses.
In modern medicine the emphasis should be placed on prophylactic treatment measures because the chance of success is much higher, the costs of treatment are lower in the case of prevention than in the case of curative treatment.
The results presented above show that urinary incontinence significantly reduce the quality of life and show that kinetic treatment helps increase perineal muscle strength, increasing the quality of life and improving or even disappearing urinary incontinence. We notice that the two groups have similar results, but the static group has had slightly better results, which can conclude that an effective kinetic treatment consists in static reeducation of the patient in the first phase for a better awareness of the perineal contraction and the transition to dynamic reeducation only when urinary incontinence improves significantly or disappears and the muscle strength improvement is stabilized. We can also conclude that physical activities should be reduced in the first phase of reeducation.
The patient›s physical or health condition does not always allow dynamic reeducation. It would be interesting to perform a long -term analysis and on a higher number of patients.
The following statements should be used “Conceptualization,
A.T. and S.T.; methodology, A.T. and S.T.; software, A.T. and S.T.; validation, A.T. and S.T.; formal analysis, A.T. and S.T.; investigation,
A.T. and S.T.; resources, A.T. and S.T.; data curation, A.T. and S.T…; writing—original draft preparation, A.T. and S.T.; writing—review and editing, A.T. and S.T.; visualization, A.T. and S.T.; supervision, A.T. and S.T., project administration, A.T. and S.T.. All authors have read and agreed to the published version of the manuscript and have equal contributions.
This research received no external funding.
Ethical review and approval number 104/25.01.2021 were obtained from UNEFS Ethics Commission.
Informed Consent Statement: Informed consent was obtained from the subject involved in the study.
The authors declare no conflict of interest.
NENCE. Neurourology and Urodynamics 37(7): 2271-2272.

This work is licensed under Creative
Commons Attribution 4.0 License
Submission Link: https://biomedres.us/submit-manuscript.php
Academia Kineperineo este lider în formarea specialiștilor în kinetoterapie, oferind cursuri de specializare și consulturi online de top. Cu o echipă de experți dedicați și un curriculum modern, suntem dedicați să te ajutăm să îți dezvolți cariera și să faci o diferență reală în viețile pacienților tăi.
Pentru o consultatie fizica in FRANTA accesati link-ul de mai jos
WhatsApp-ne
